Your material is “medical grade.” So why did it fail?
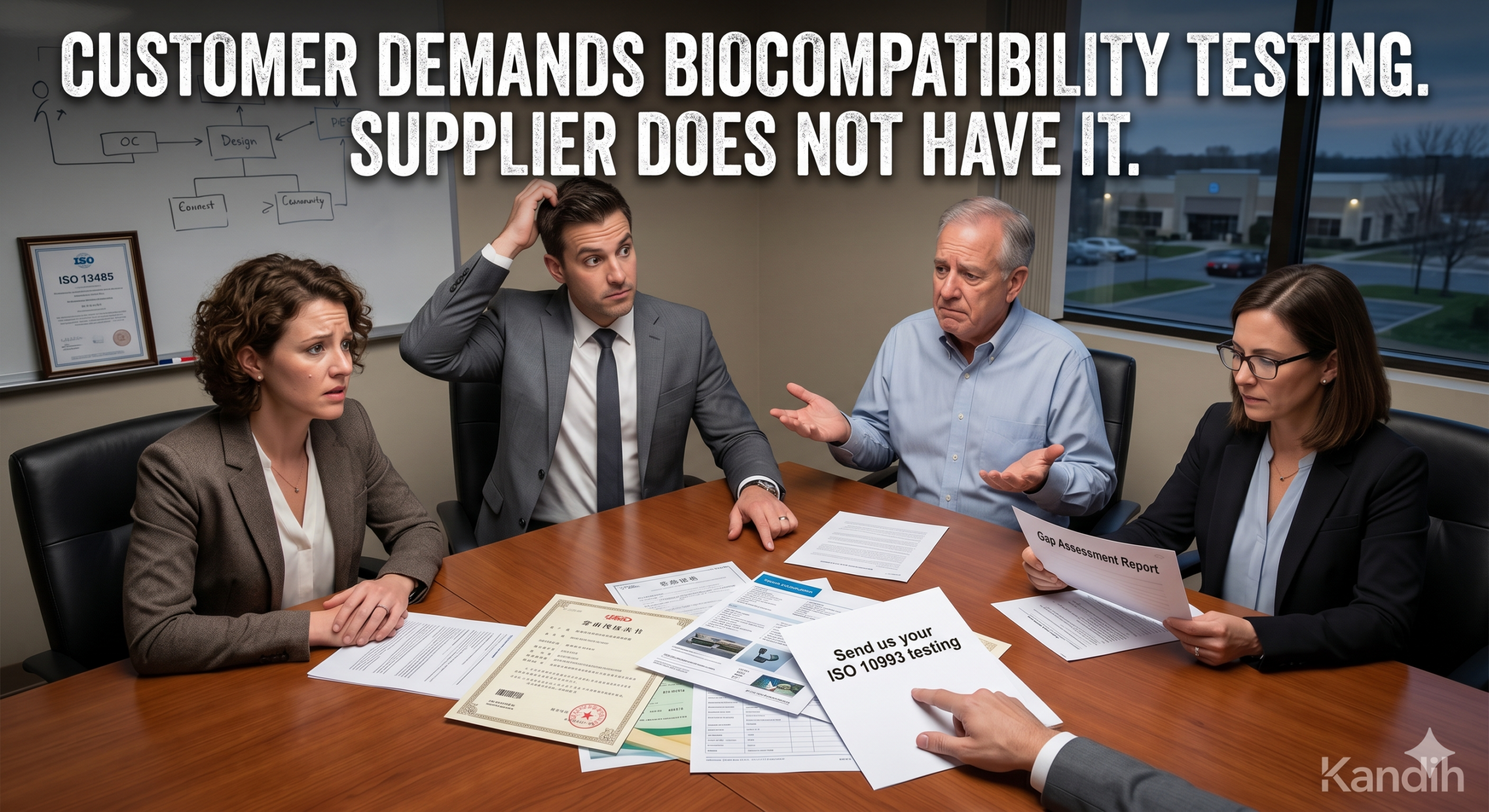
Biocompatibility Testing: When Customers Demand It But Suppliers Don’t Have It
April 27, 2026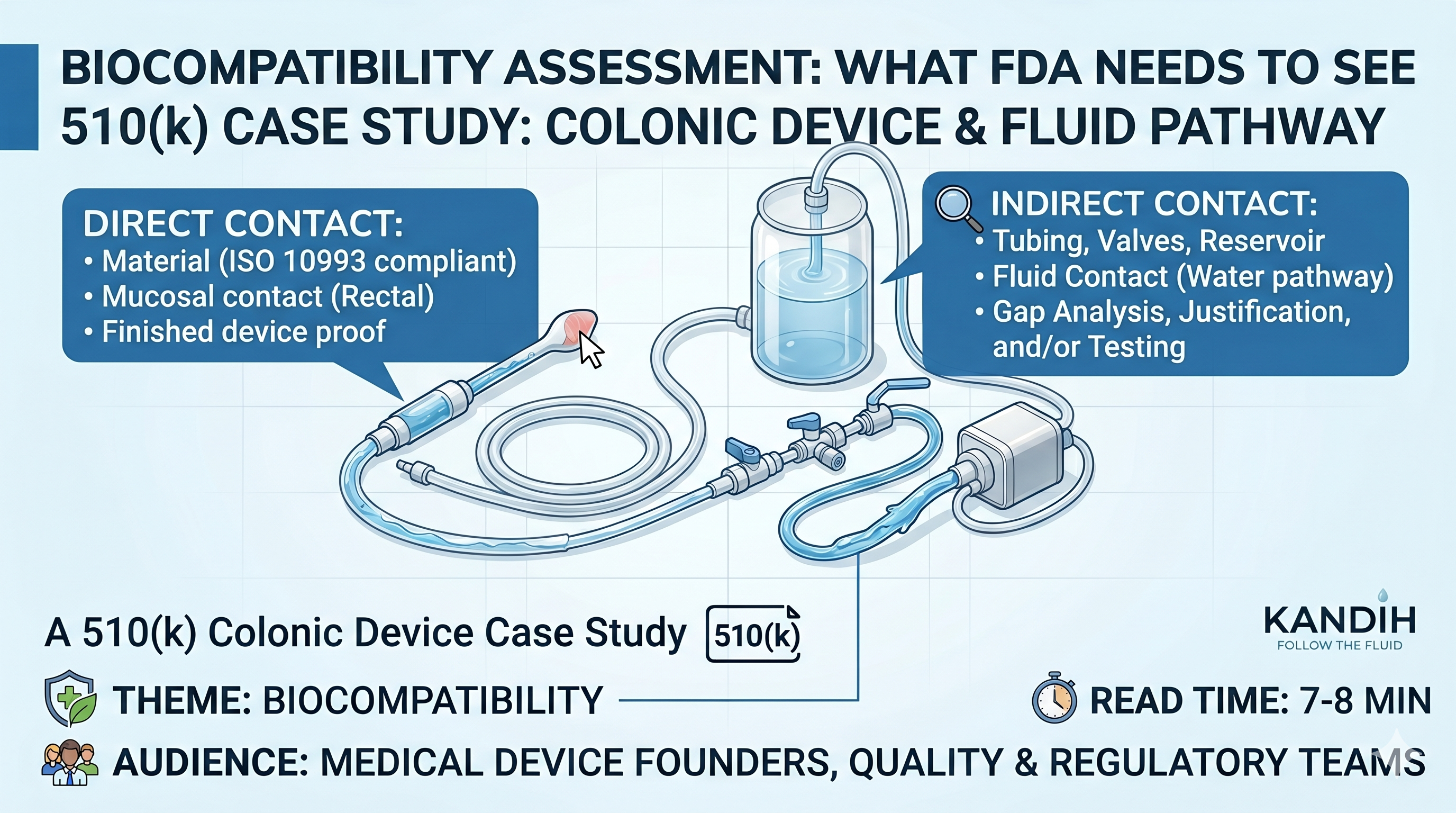
Direct vs. Indirect Contact in ISO 10993: A 510(k) Colonic Device Case
May 11, 2026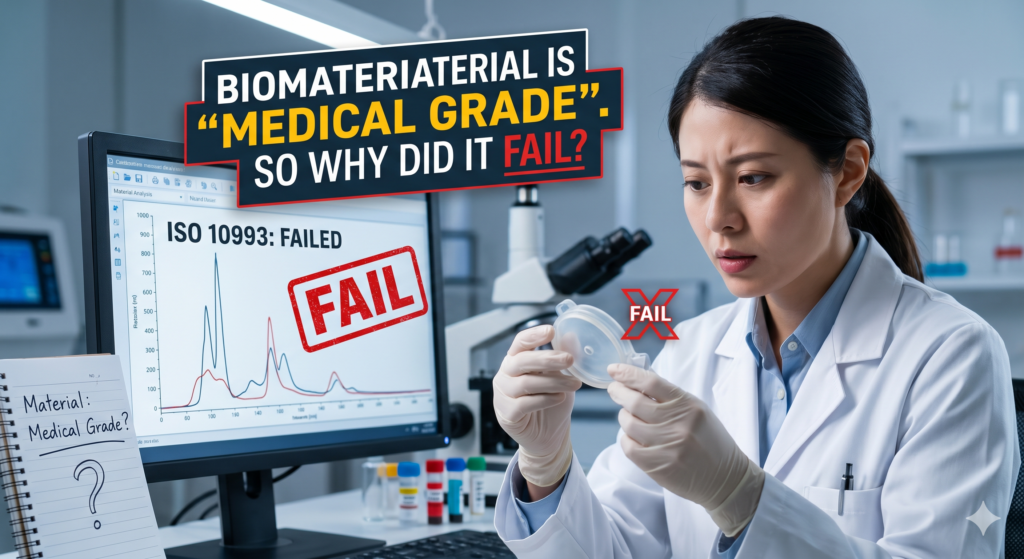
A device that passes material inspection can still fail ISO 10993 biocompatibility testing — and understanding why the difference between a delay and a disaster is.
Kandih Regulatory Insights ·
The team thought this would be easy. The material was “medical grade.” The supplier had used it in healthcare for years. The device seemed simple enough, and the regulatory plan looked clean.
Then the biocompatibility results came back. Fail. Not a minor clarification — a real failure. The kind that makes everyone suddenly interested in chemistry, sterilization, and every tiny material choice nobody questioned during development.
“But the material is medical grade. How did it fail?”
That question starts the ISO 10993 adventure. And like most adventures, it begins with a false sense of safety.
The myth of the magic label
“Medical grade” sounds powerful. It feels like a regulatory shortcut — a safety shield that should make test failures disappear. But in practice, it means surprisingly little on its own.
Material can be suitable for some medical uses and still fail in your device. The final product is not just the raw material. It is the raw material plus the design, manufacturing process, additives, surface treatments, sterilization, packaging, storage conditions, and intended use. Biocompatibility is not a personality trait. It is a product-specific conclusion.
ISO 10993 evaluates biological safety based on the finished device — its body contact, contact duration, materials, processing, sterilization, packaging, and potential chemical release. Not just the raw material that went into it.
Eight reasons medical-grade materials still fail
A test failure does not always mean the base material is bad. Often, something changed between “raw material” and “finished device.” Here are the most common culprits.
| 01 Additives Plasticizers, stabilizers, pigments, and curing agents can leach out — even if the base polymer is familiar. | 02 Colorants A blue device and a clear device made from the same base polymer may not share the same biological profile. |
| 03 Adhesives & coatings The patient-contacting surface may be a coating or adhesive residue, not the main material at all. | 04 Manufacturing residues Mold release agents, solvents, and lubricants may not appear on the BOM but show up in biological tests. |
| 05 Sterilization Ethylene oxide residuals, radiation-induced degradation, or heat effects can alter the device’s biological profile. | 06 Supplier changes “Same material” can mean a new resin source, additive package, cleaning process, or manufacturing site. |
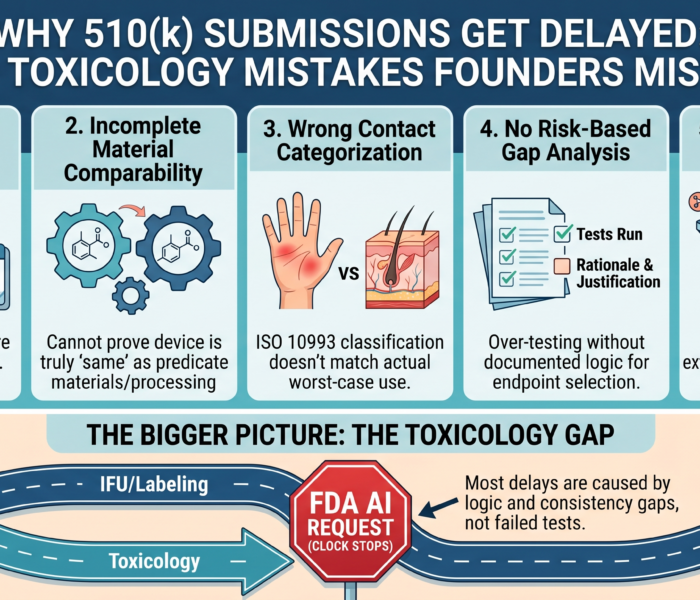
| 07 Wrong test article Testing a prototype instead of the production device, or testing pre-sterilization, can give misleading results. | 08 Misclassified contact A device classified as ‘external’ may still contact mucosal tissue, damaged skin, or a patient’s fluid path. |
What to do after an unexpected failure
The wrong instinct is to panic-order every test available. That is an expensive way to create more confusion. A smart response starts with methodical investigation.
| 1 | Confirm the failure Review the test method, sample description, extraction conditions, controls, and lab deviations. Not every surprising result is a valid one. |
| 2 | Map every material and process Document all patient-contacting materials, adhesives, colorants, lubricants, cleaning agents, sterilization method, and packaging. Many teams discover here that their materials file was never complete. |
| 3 | Identify likely root causes Was there a new pigment? A supplier change? Sterilization residue? A mismatch between prototype and production? The goal is to find the source of biological risk, not to blame the lab. |
| 4 | Decide on targeted next steps Chemical characterization can identify what is extracted from the device. A toxicological risk assessment can then determine whether those chemicals present unacceptable risk — far more useful than blindly repeating the same failed test. |
| 5 | Update the Biological Evaluation Report Document what failed, why, what investigation was done, what was found, and what corrective action was taken. An unexplained failure is far more dangerous than an explained one. |
Hope is not a test strategy. It is just anxiety in a lab coat.
Why this matters more for startups and importers
For startups, unexpected biocompatibility failures can damage timelines, budgets, and investor confidence simultaneously. For importers, the risk is compounded because the supplier often lacks full material data or process transparency.
A supplier saying “we have sold this for years” is not evidence. You need documentation for your device, your market, your intended use, and your quality file. Hospitals, distributors, and OEM partners increasingly ask for biocompatibility documentation before purchase — and “the supplier said it is medical grade” will stall the deal.
The bottom line
Medical-grade materials can still fail ISO 10993 testing — and that is not the end of the story. Handled poorly, failure becomes a delay, a budget problem, and a trust problem. Handled well, it becomes a stronger product file, a better supplier strategy, and a more defensible path to market. In medical devices, “medical grade” may open the door. Evidence keeps you in the room.
References

{kind=link}
{kind=link}
{kind=link}