Biocompatibility Testing: When Customers Demand It But Suppliers Don’t Have It

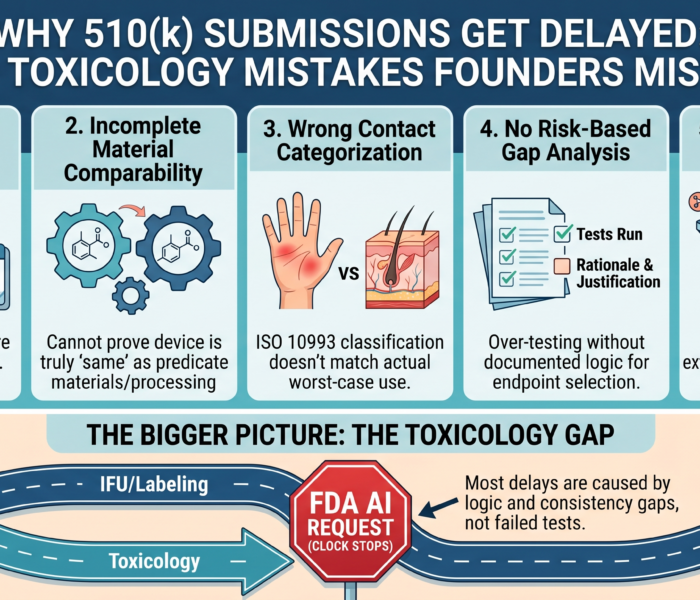
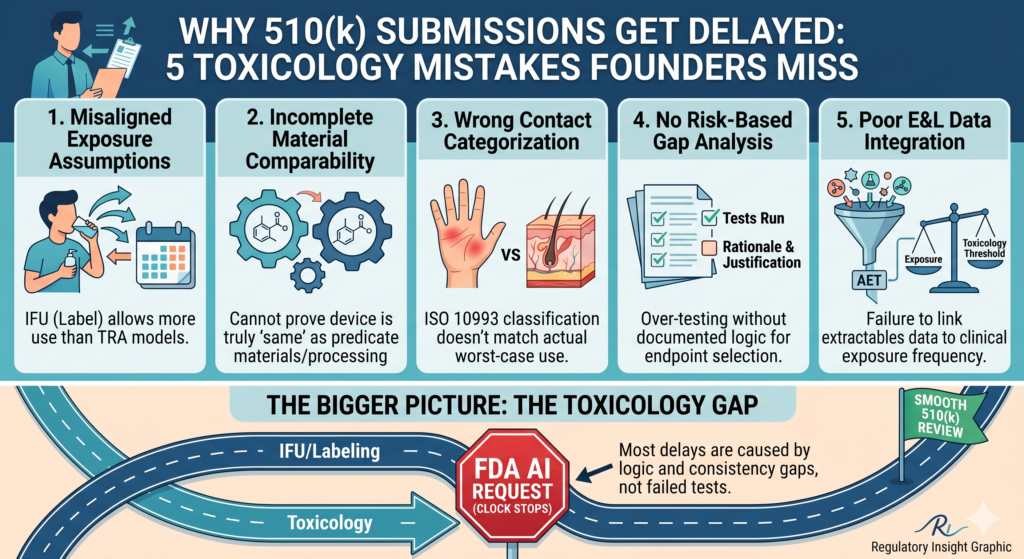
Why 510(k) Submissions Get Delayed: 5 Toxicology Mistakes Founders Miss
April 24, 2026
Your material is “medical grade.” So why did it fail?
May 4, 2026
Imported Class I Device Lacks Testing: What Now?
A founder imports a simple Class I medical device.
No electronics.
No software.
No implant.
No dramatic risk profile.
The supplier says, “This product has been sold for years.”
The customer says, “Send us your biocompatibility testing.”
Then the room gets quiet.
The supplier does not have ISO 10993 testing. They do not have a biological evaluation report. They may have a material safety data sheet, a certificate of analysis, or a “medical grade” claim from a raw material vendor. But they do not have a real biocompatibility package.
Now the importer has a problem.
Not because every Class I device automatically needs a full laboratory test panel. That is not how biocompatibility works.
The problem is simpler: the customer is asking a safety question, and the supplier cannot answer it with evidence.
That gap can delay sales, weaken distributor confidence, trigger regulatory questions, and expose the company to risk if the device contacts the body.
Executive Summary
Biocompatibility is not just a box to check when FDA asks for it. It is the process of showing that a medical device is biologically safe for its intended contact with the human body.
For medical devices, ISO 10993-1 is the main framework used to evaluate biological safety through a risk management process. FDA’s biocompatibility guidance explains how ISO 10993-1 can support FDA submissions, including 510(k), PMA, IDE, HDE, and De Novo applications. Even when a Class I device is exempt from premarket notification, the device is still subject to FDA general controls, including requirements related to safety, labeling, registration, records, and adulteration or misbranding.
The key point: Class I does not mean “no evidence needed.”
It means the regulatory pathway may be lighter. The safety obligation does not disappear.
The Real-World Problem: “Our Customer Wants Biocompatibility”
This situation is common with imported devices.
A U.S. company finds a supplier overseas. The product looks simple. The price works. The market need is real.
Then a hospital, distributor, clinic, purchasing group, or private-label partner asks:
“Can you provide biocompatibility testing?”
The importer goes back to the supplier.
The supplier sends:
- a CE certificate that may not apply to the exact product
- an ISO 13485 certificate for the factory
- a raw material data sheet
- a certificate saying the product is “non-toxic”
- a test report for a different model
- a letter saying the material is “medical grade”
- nothing useful at all
This is where companies often make the wrong move.
They either panic and order every ISO 10993 test on the menu, or they ignore the request and hope the customer moves on.
Both are bad strategies.
Biocompatibility should be handled like a risk question, not a shopping list.
What Is Biocompatibility Testing?
Biocompatibility testing checks whether a medical device, material, chemical residue, or manufacturing-related substance could cause harm when the device contacts the body.
The risk depends on:
- what the device touches
- how long it touches the body
- what materials are used
- how the device is manufactured
- whether chemicals can leach out
- whether the device is sterile or non-sterile
- whether the device is single-use or reusable
- whether the user is a patient, clinician, or both
A skin-contact device is different from a blood-contact device. A device used for a few minutes is different from one used for days. A device that contacts intact skin is different from one that contacts mucosal tissue, breached tissue, circulating blood, or implanted tissue.
That is why ISO 10993-1 starts with device contact type and contact duration. The goal is to evaluate biological risk in a structured way, not blindly run tests.
Does a Class I Device Need Biocompatibility Testing?
Sometimes yes. Sometimes no.
A Class I device may not need a full biocompatibility test panel if the manufacturer can justify biological safety using existing information. But the company still needs a defensible rationale.
That rationale may include:
- confirmed material identity
- supplier material specifications
- prior safe use of the same materials
- manufacturing process information
- chemical characterization
- toxicological risk assessment
- comparison to a legally marketed device
- existing biological test data
- clinical history or complaint history
- evidence that the device has no direct or indirect body contact
The important word is defensible.
A customer may not accept “our supplier says it is safe.”
FDA will not be impressed by “we think it is fine.”
Investors will not love “we did not ask.”
A proper biological evaluation explains why testing is needed, why testing is not needed, or why existing data are enough.
The Mistake Importers Make
Many importers assume the foreign supplier owns the problem.
They do not.
If your company is placing the device on the U.S. market, your company needs to understand whether the product is compliant and safe for its intended use.
Imported medical devices must meet U.S. requirements. A low-risk classification does not erase the need for appropriate documentation, truthful labeling, supplier controls, complaint handling, and risk management.
The supplier may manufacture the device, but the importer carries commercial and regulatory risk.
That is the part many early-stage companies miss.
They treat the supplier as the evidence holder. But in practice, the supplier may only be a factory, not a regulatory partner.
“Medical Grade” Is Not a Biocompatibility Strategy
“Medical grade” sounds comforting.
It is also often meaningless unless it is supported by specific evidence.
A material can be called medical grade and still be inappropriate for the finished device. Why? Because biological safety depends on more than the raw material.
It also depends on:
- colorants
- additives
- adhesives
- lubricants
- mold release agents
- processing aids
- cleaning residues
- sterilization effects
- packaging interactions
- degradation products
- surface treatments
- manufacturing changes
The finished device is what touches the patient or user.
That means the finished device matters.
A raw material certificate can support the file, but it does not automatically prove the finished device is biocompatible.
That is like saying flour is safe, so the whole cake must be safe. Maybe. But let’s not ignore what else went into the batter.
What Should You Do When the Supplier Has No Testing?
Start with a structured gap assessment.
Do not begin with the lab. Begin with the device.
1. Confirm the exact device identity
You need to know whether the product being sold matches the product described in any documents.
Check:
- model number
- material composition
- manufacturing site
- supplier name
- packaging
- sterilization status
- labeling
- intended use
- body contact type
- duration of contact
- accessories and patient-contacting components
A test report for a similar device may not be enough.
Similar is not the same as identical.
2. Define the nature and duration of body contact
This is the backbone of the biological evaluation.
Ask:
- Does it contact the body directly?
- Does it contact intact skin?
- Does it contact mucosal membranes?
- Does it contact blood?
- Does it contact breached or compromised tissue?
- Is contact limited, prolonged, or permanent?
- Is there indirect contact through fluids or gas pathways?
This step determines which biological endpoints may be relevant.
3. Collect all available supplier information
Request:
- bill of materials
- material specifications
- colorant and additive information
- manufacturing process overview
- sterilization information, if applicable
- cleaning process information
- packaging materials
- existing test reports
- certificates of analysis
- supplier change history
- complaint or adverse event history
- evidence of prior market use
If the supplier cannot provide basic material information, that is not a paperwork issue. That is a supplier qualification issue.
4. Build a Biological Evaluation Plan
A Biological Evaluation Plan outlines how biological safety will be assessed.
It should explain:
- the device description
- patient-contacting materials
- body contact category
- contact duration
- relevant biological endpoints
- available data
- data gaps
- whether testing is needed
- justification for any endpoints not tested
This prevents random testing.
It also gives customers and auditors a clear story.
5. Decide whether testing is actually needed
Testing may be needed when there are real data gaps.
Common endpoints may include cytotoxicity, sensitization, irritation or intracutaneous reactivity, systemic toxicity, material-mediated pyrogenicity, chemical characterization, or other endpoints depending on the device.
But testing should match the risk.
A device with limited intact-skin contact should not be treated like an implant. A reusable mucosal-contact device should not be treated like a sticker.
The job is to match evidence to exposure.
6. Create a Biological Evaluation Report
The Biological Evaluation Report is the final risk-based argument.
It pulls together the data and explains whether the device is biologically safe for its intended use.
A strong report does not just say, “Testing passed.”
It says:
- what was evaluated
- what evidence was used
- what gaps were identified
- how risks were addressed
- what conclusions were reached
- what limitations remain
- what must be controlled going forward
This becomes the document customers actually need.
What If the Customer Demands Testing Anyway?
Sometimes the customer’s requirement is stricter than the regulation.
That is business reality.
A distributor may require testing before onboarding. A hospital may require it for value analysis. A private-label partner may want it for their own quality file. A larger company may not accept a risk rationale without lab data.
In those cases, you have three options.
First, provide a scientifically justified biological evaluation and explain why testing is not needed.
Second, perform targeted testing to close specific gaps.
Third, walk away if the supplier cannot support the product and the commercial opportunity does not justify the cost.
The worst option is pretending the gap does not exist.
Customer trust is hard to win and very easy to vaporize.
Why This Matters for Imported Devices
Imported Class I devices can look deceptively simple.
The regulatory entry point may be easier than a Class II or Class III device. But the commercial burden can still be serious.
Customers may ask for documentation before they buy. Insurers, distributors, and group purchasing organizations may ask for evidence. FDA may inspect records. A complaint may force the company to explain how safety was assessed.
If the file is empty, the company has little room to maneuver.
That is why biocompatibility is not just a testing issue. It is a market access issue.
No evidence, no confidence. No confidence, no purchase order.
Where Kandih Comes In
Kandih helps medical device companies turn supplier uncertainty into a clear, defensible biocompatibility strategy.
For imported Class I devices, Kandih can help determine whether the device needs testing, whether existing information is enough, and what documentation is missing. The goal is not to over-test. The goal is to build the right evidence package for the device, the customer, and the regulatory risk.
Kandih supports:
- biocompatibility gap assessments
- supplier documentation reviews
- ISO 10993 endpoint mapping
- Biological Evaluation Plans
- Biological Evaluation Reports
- test strategy development
- customer-response documentation
- regulatory risk review for imported devices
- support for FDA-facing or investor-facing documentation
This is especially useful when a customer is asking for biocompatibility testing, but the supplier does not have it.
Kandih helps answer the hard questions:
- Is testing actually required?
- What evidence already exists?
- Can we justify biological safety without new testing?
- What testing would close the gap fastest?
- Is the supplier too risky to rely on?
- What should we tell the customer?
- What documentation should be in the quality file?
The point is not to make the file look pretty.
The point is to make the file survive questions.
AEO Quick Answer: What Should You Do If a Supplier Has No Biocompatibility Testing?
If a supplier has no biocompatibility testing, do not immediately order a full ISO 10993 test panel. First, confirm the device’s body contact type, contact duration, materials, manufacturing process, and available supplier data. Then complete a biological evaluation gap assessment. If existing evidence is not enough, perform targeted testing or chemical characterization based on the device’s actual biological risk.
Final Takeaway
When a customer asks for biocompatibility testing, they are really asking:
“Can you prove this device is safe for body contact?”
If the supplier cannot answer, the importer must.
For Class I devices, the answer may be simple. But it still needs to be documented.
A strong biocompatibility strategy protects more than regulatory compliance. It protects customer trust, sales momentum, supplier decisions, and the company’s reputation.
Because in medical devices, “low risk” does not mean “no risk.”
And “the supplier said it was fine” is not a strategy.
References
- FDA — Use of International Standard ISO 10993-1, “Biological evaluation of medical devices — Part 1: Evaluation and testing within a risk management process”
https://www.fda.gov/regulatory-information/search-fda-guidance-documents/use-international-standard-iso-10993-1-biological-evaluation-medical-devices-part-1-evaluation-and - FDA — Recognized Consensus Standards: ISO 10993-1 Biological Evaluation of Medical Devices
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfStandards/detail.cfm?standard__identification_no=46606 - ISO — ISO 10993-1: Biological evaluation of medical devices — Part 1
https://www.iso.org/standard/68936.html - eCFR — 21 CFR § 860.3: Medical Device Classification Definitions
https://www.ecfr.gov/current/title-21/chapter-I/subchapter-H/part-860/subpart-A/section-860.3 - eCFR — 21 CFR Part 860: Medical Device Classification Procedures
https://www.ecfr.gov/current/title-21/chapter-I/subchapter-H/part-860

{kind=link}
{kind=link}
{kind=link}