CGM Sensors and Hidden Plasticizers: Reddit’s CGM Material Fears
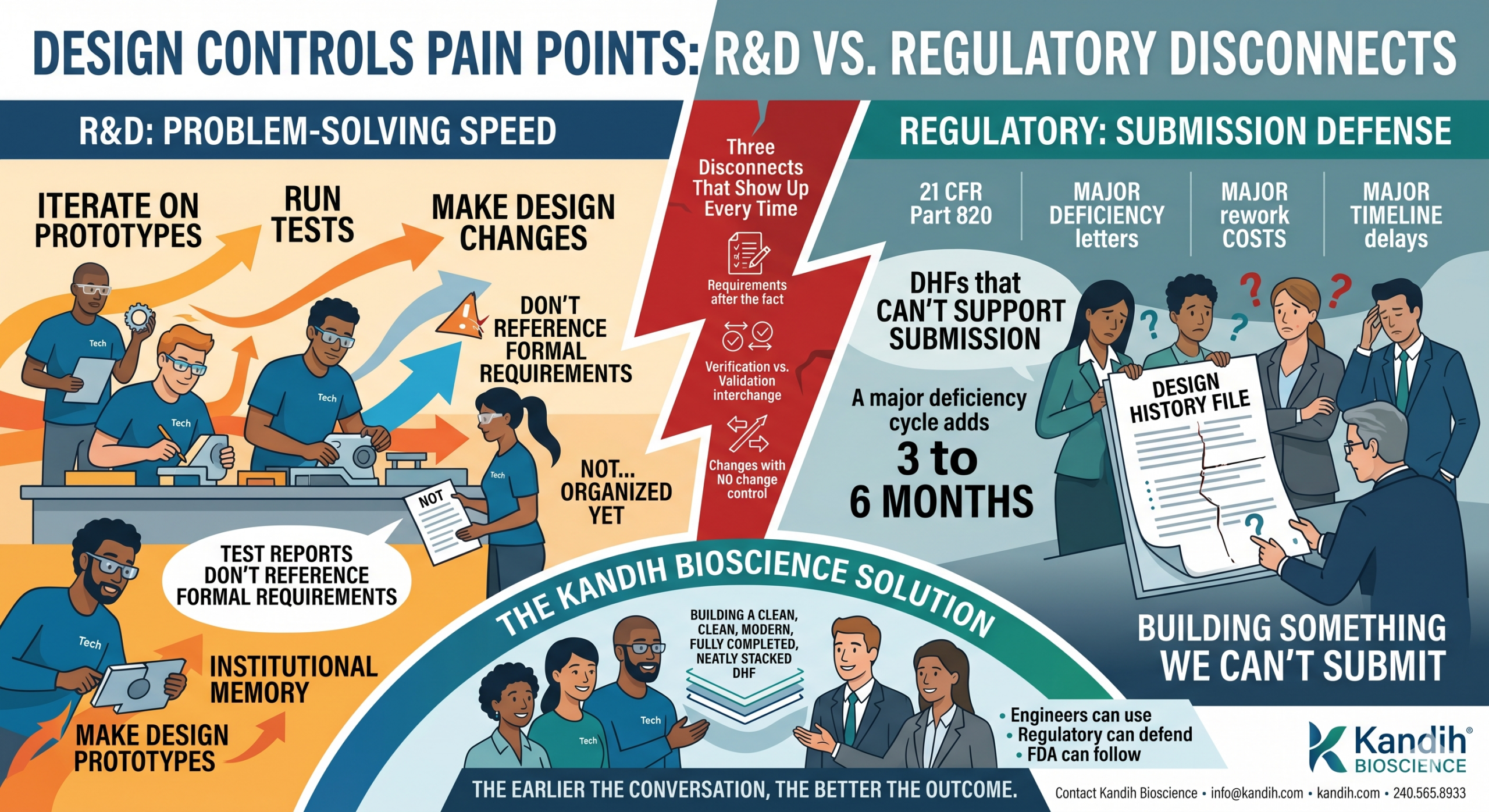
Design Controls Pain Points: R&D vs. Regulatory Disconnects
June 15, 2026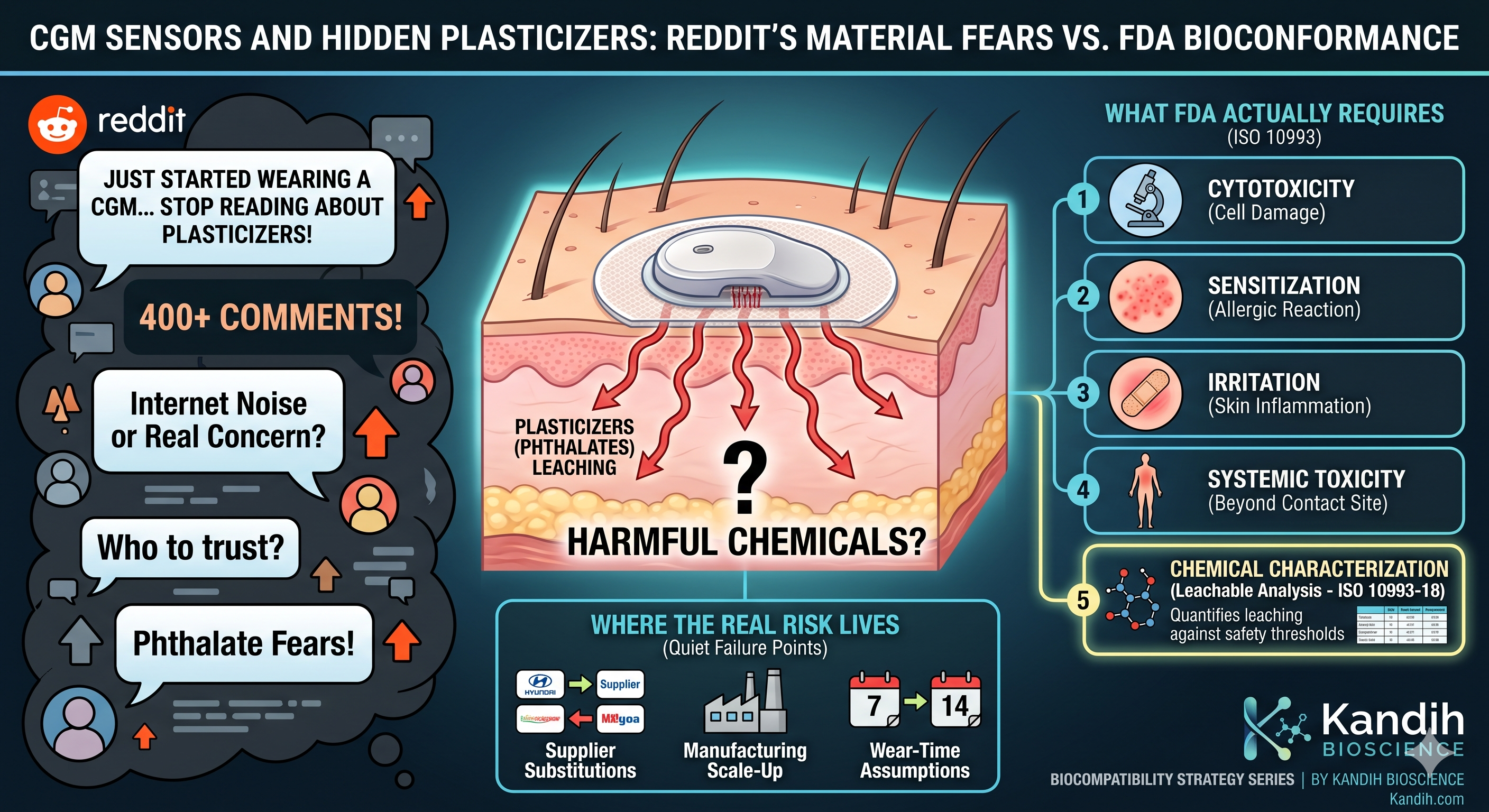
By Kandih Bioscience • Biocompatibility Strategy Series
From r/prediabetes: “I just started wearing a CGM and now I can’t stop reading about plasticizers in the adhesive. Is this actually something I should worry about, or is it just internet noise? Genuinely don’t know who to trust here.”
That thread has over 400 comments. Some are reasonable. Some are not. A lot of them cite studies nobody actually linked, or repeat a claim that started somewhere else and got passed along until it sounded like fact.
This is a real concern with a confusing answer, and most of what’s online doesn’t actually explain how CGM materials get evaluated before they reach a patient’s arm.
If you’re a founder building a CGM or a wearable biosensor — or an investor trying to figure out whether a company’s materials strategy is actually sound — this is the conversation that’s happening about your product right now, in forums you’re probably not reading. It’s worth understanding what’s true, what’s not, and what FDA actually requires before any of this reaches a patient.
What People Are Actually Worried About
Strip away the noise and the concern usually comes down to one thing: plasticizers.
Plasticizers are chemicals added to plastics and adhesives to make them flexible. Some plasticizers — particularly a class called phthalates — have been linked in some studies to hormone disruption when they leach out of a material and enter the body in meaningful quantities.
That’s a legitimate area of toxicology. It’s also a topic that gets flattened online into something much scarier and much less precise than the actual science.
A CGM sensor sits on the skin, usually for 10 to 14 days, with an adhesive patch and a small filament that sits just under the skin. That’s sustained skin contact and a minor break in the skin barrier — both of which matter for how a device gets evaluated.
The question patients are really asking is: how do I know the plastic and adhesive in this thing won’t leach something harmful into my body over two weeks of continuous wear?
It’s a fair question. And there’s a real, FDA-regulated answer to it — it’s just not the answer most Reddit threads give.
What FDA Actually Requires Before a CGM Reaches Skin
A CGM is classified by FDA as a device with prolonged skin contact — and depending on the filament design, sometimes breached or compromised skin contact too, because the sensor filament sits under the skin surface.
That classification triggers a specific set of biocompatibility requirements under ISO 10993, the international standard FDA uses to evaluate medical device materials. For a device like this, manufacturers are expected to evaluate:
- Cytotoxicity — does the material damage or kill living cells on contact
- Sensitization — does repeated exposure trigger an allergic or immune response
- Irritation — does the material cause inflammation or skin reaction at the contact site
- Systemic toxicity — could chemicals from the device cause effects beyond the contact site if absorbed
- Chemical characterization — a detailed analysis of exactly what chemicals could leach from the device under realistic wear conditions, including plasticizers, adhesives, and any residual manufacturing chemicals
That last one — chemical characterization, covered under ISO 10993-18 — is exactly the test that answers the plasticizer question directly. It identifies and quantifies what’s actually capable of leaching from the device, then compares those amounts against established safety thresholds for human exposure.
This isn’t a one-time check box. It has to reflect the device as it will actually be worn — same materials, same adhesive formulation, same sterilization method, same wear duration. A change to any of those after testing can invalidate the original data.
This is the answer most online discussions skip entirely: a CGM cannot legally reach the U.S. market without documented evidence that its materials — plasticizers included — were evaluated for exactly the leaching concern patients are worried about. The system isn’t perfect, but it’s not the regulatory void that online fear implies.
Where the Real Risk Actually Lives
Here’s the part that doesn’t get said enough: the danger isn’t that biocompatibility testing doesn’t exist. It’s that companies sometimes treat it as a one-time checkbox instead of an ongoing discipline tied to every material and manufacturing decision.
This is where founders building CGMs and similar wearables actually run into trouble — not because they skip testing outright, but because of three quieter failure points:
Supplier substitutions without retesting.
A company tests their adhesive, gets clean biocompatibility results, and ships. Eighteen months later, their adhesive supplier changes their formulation — maybe to cut cost, maybe due to a supply chain issue — and nobody flags it as a material change requiring new testing. The original data no longer reflects what’s actually on the patient’s skin.
Manufacturing scale-up changes the chemistry.
A material that passed testing at small-batch production scale can behave differently once you’re manufacturing at volume. Curing times, temperatures, and process conditions can all shift residual chemical content. If the validation data was only ever generated on prototype-scale units, it may not represent what’s shipping.
Wear-time assumptions that don’t match real use.
If a sensor is tested for a 7-day wear cycle but later approved or marketed for 14-day wear, the original chemical characterization data may not account for the additional leaching that happens over the extra week. Extending wear time without re-evaluating biocompatibility is a real gap, and it’s one regulators specifically look for.
None of these are exotic scenarios. They’re common, quiet failure points that happen because biocompatibility gets treated as something you do once at the start, instead of something you revisit every time a material, supplier, or use condition changes.
What This Means If You’re a Founder
If you’re building a CGM, a wearable biosensor, or any device with sustained skin contact, the plasticizer conversation happening on Reddit is a preview of the conversation your customers will eventually have about your product — whether you participate in it or not.
That makes two things matter more than they might seem to early in development:
- Your chemical characterization data needs to be tied to your actual production materials and process — not your prototype. If your supplier, formulation, or manufacturing scale changes, that data needs to be revisited, not assumed to still apply.
- Your wear-time claims need to match your testing. If you’re marketing 14-day wear, your biocompatibility data needs to reflect 14 days of realistic leaching conditions — not the 7-day data from an earlier design phase.
Being able to answer the plasticizer question directly — not defensively, not vaguely — is a real differentiator. Patients are asking. Increasingly, so are reporters, advocacy groups, and regulators paying attention to consumer-facing health tech.
Founders who can explain, in plain language, exactly what their device’s chemical characterization data shows — and why their wear-time claims are backed by it — build more trust with patients and with FDA than founders who simply say ‘we passed ISO 10993.’ The detail is the credibility.
What This Means If You’re an Investor
If you’re evaluating a CGM or wearable biosensor company, the plasticizer question is a useful, specific due diligence probe — because the answer tells you a lot about how seriously the team treats ongoing biocompatibility risk, not just initial testing.
A few direct questions worth asking:
- Has your chemical characterization data been updated to reflect your current production materials and supplier list — not just your original prototype?
- If you’ve changed adhesive suppliers, materials, or manufacturing scale since your last biocompatibility testing, has that triggered a re-evaluation?
- Does your wear-time labeling match the wear duration your chemical characterization data actually covers?
A team that answers these clearly, with specifics, has almost certainly built biocompatibility into their quality system as an ongoing process. A team that responds with ‘we passed our testing’ and stops there hasn’t demonstrated that the data is still current — and that gap can resurface later as a regulatory or reputational risk, sometimes after a product is already on the market.
Where Kandih Bioscience Comes In
The plasticizer conversation happening online isn’t going away, and it shouldn’t. Patients wearing a device on their skin for two weeks at a time deserve a real, specific answer — not a vague reassurance.
At Kandih Bioscience, we help CGM and wearable biosensor companies build biocompatibility programs that hold up to that level of scrutiny — from FDA, from investors, and increasingly from patients themselves. That includes:
- Designing a chemical characterization strategy under ISO 10993-18 that’s tied to your actual production materials, adhesive formulation, and wear-time claims
- Building a change-control process that flags supplier substitutions, formulation changes, and manufacturing scale-up as biocompatibility triggers — not just engineering decisions
- Reviewing existing biocompatibility data to confirm it still reflects what’s shipping today, not what was tested at an earlier development stage
- Preparing clear, plain-language documentation your team can use to answer patient and investor questions directly, without hedging
If you’re a founder who wants to know whether your current biocompatibility data actually supports your product as it exists today, that’s a conversation worth having before it becomes a question you have to answer publicly.
If you’re an investor who wants a plain-language read on a CGM or wearable company’s materials risk, we can walk through exactly what to look for.
Contact Kandih Bioscience • info@kandih.com • kandih.com • 240.565.8933
References
1. FDA — Use of International Standard ISO 10993-1: Biological Evaluation of Medical Devices (2020)
3. FDA — Biocompatibility of Medical Devices: Overview and FDA’s Approach (2021)
4. National Institute of Environmental Health Sciences — Phthalates Overview (2023)
5. FDA — Continuous Glucose Monitoring Systems: Device Classification and Premarket Requirements (2023)
6. FDA — Guidance on the Use of ISO 10993-10: Tests for Skin Sensitization (2023)