By Harriet Kamendi | Regulatory Toxicologist | Kandih Group
Imagine you are a founder. You have compelling efficacy data, a clean mechanism
of action, and enough runway to file an IND. Your investors are excited. Your
scientific advisory board is aligned. And your toxicology package consists of a
single 28-day rat study and a literature review.
You are not unusual. In the biotech ecosystem, this scenario plays out constantly
— not because founders are reckless, but because toxicology is systematically
treated as a compliance exercise rather than a strategic function. It gets done
because the FDA requires it, not because the team understands what it is actually
answering.
What toxicology actually answers is this: given what we know about how this
compound behaves in the body, across what doses, durations, and populations,
can we responsibly put it into humans — and what will kill this program if we get
it wrong?
No other discipline asks all of those questions at once. That is not an accident. It
is architecture.
Why “the whole system” — and why only toxicology?
The claim in this title is intentionally strong, and it deserves a direct defense.
Competing disciplines also claim systemic views:
- Systems biology integrates molecular pathways and network dynamics.
- Epidemiology integrates population-level outcomes and environmental
exposures. - Pharmacology integrates mechanism of action and dose–response for
intended effects. - Environmental health science integrates exposure with ecological risk.
Each of these is powerful within its domain. But none of them is structurally
required to produce a governance-ready answer. Epidemiology needs widespread
human exposure before it can speak at all. Systems biology produces mechanistic
insight but not a margin of safety. Pharmacology describes what a drug does
when it works, not what it does when it fails — and not under the exposure
conditions regulators actually care about.
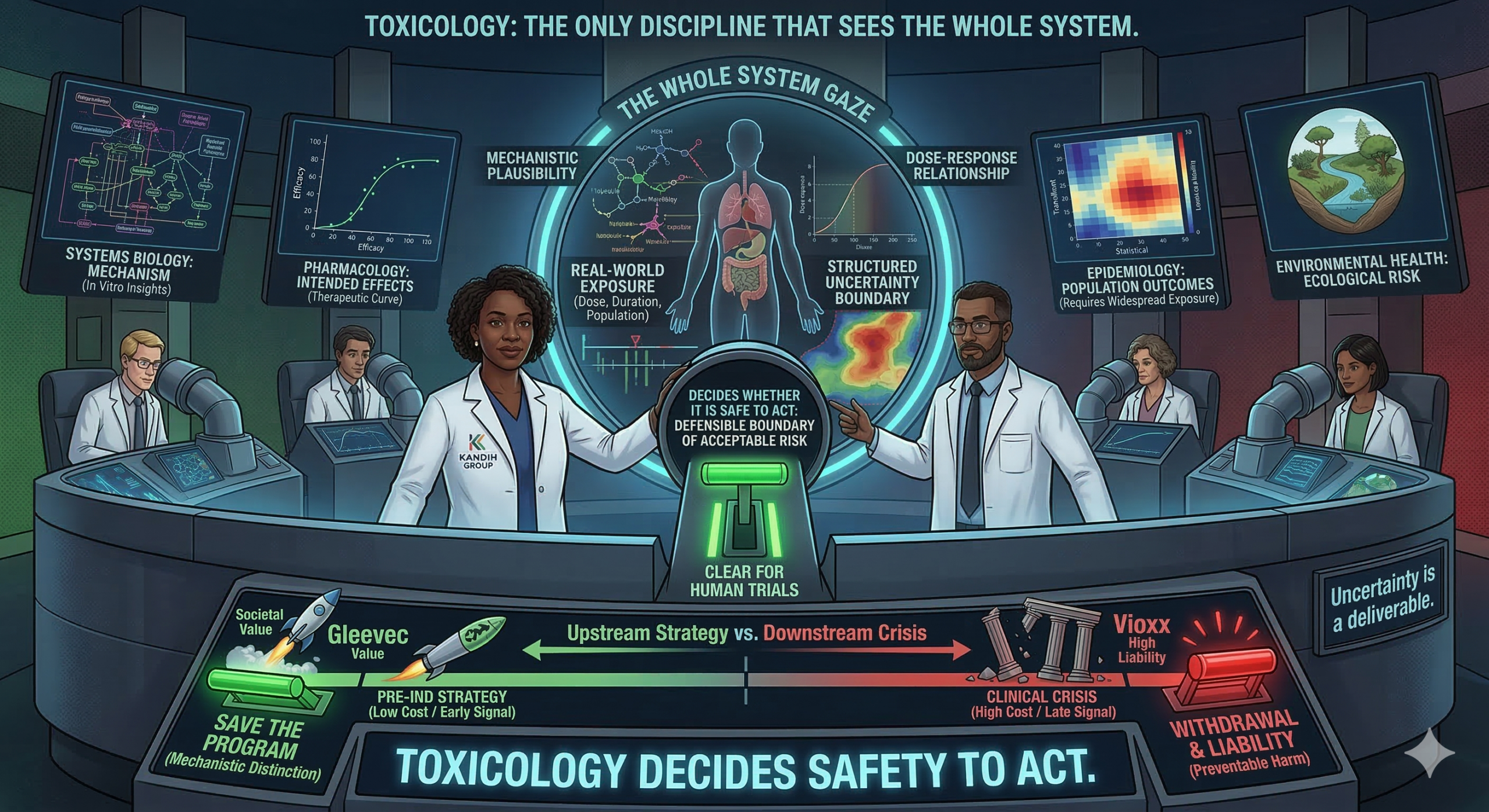
Toxicology is uniquely architected to combine all four elements that
governance requires: mechanistic plausibility, dose–response relationship, real-
world exposure conditions (how much, how often, for how long), and structured
uncertainty that can be explicitly documented and carried forward to a decision.
The canonical framework — hazard identification, dose–response assessment,
exposure assessment, risk characterization — is not a bureaucratic checklist. It is
a decision engine. The output is not just “this compound is harmful.” The output
is: here is what we know, here is what we do not know, here are the assumptions
we have made, and here is the defensible boundary of acceptable risk.
Other disciplines describe the system. Toxicology decides whether it is
safe to act on it.
The economics make this argument for you
For investors and founders, the governance argument eventually needs to land as
a financial argument. Here it is.
According to the Congressional Budget Office, clinical trials account for more
than twice the R&D spend of preclinical research on a per-approved-drug basis —
roughly $1.065 billion in average clinical trial spending per approved new drug.
Phase III alone absorbs hundreds of millions, and approximately half of all Phase
III trials fail. The overall clinical success rate from IND to approval sits between
10 and 14 percent, depending on therapeutic area.
The implication is direct: every dollar of toxicology-related risk that passes
through IND unexamined gets repriced in clinical-stage dollars — with a
multiplier. A compound-stopping safety signal that surfaces in a two-week in
vitro assay costs almost nothing to act on. The same signal surfacing in a Phase II
trial has already consumed tens of millions, triggered regulatory correspondence,
and may have exposed trial participants to a preventable harm. The same signal
surfacing post-approval has a different name: liability.
Vioxx is the reference case. Rofecoxib was approved in 1999 and became one
of the most prescribed medications in the world. Cardiovascular risk signals,
present in early clinical data and mechanistically plausible from COX-2 pathway
biology, were not acted on as a stop/go criterion. Merck voluntarily withdrew the
drug in 2004 after an estimated 20 million Americans had taken it. The financial
reckoning: $4.85 billion in product liability settlements, $950 million in DOJ
criminal charges for improper marketing, and $830 million in securities class
action payments — a total liability exceeding $6.8 billion. None of that accounts
for the brand damage, the decade of litigation management, or the lives affected.
Merck did not fail to run toxicology. They failed to integrate mechanistic
cardiovascular signals into their governance logic early enough to prevent a
clinical and commercial catastrophe. That is a toxicology problem, but more
precisely it is a governance problem: toxicology was downstream of commercial
momentum rather than upstream of it.
What it looks like when toxicology works: the Gleevec story
The failure cases are instructive. But thought leadership that only tells disaster
stories creates the wrong frame: toxicology as a series of things that went wrong
somewhere else, to someone else, at a scale you do not recognize. So let us look at
what right looks like.
In 1996, Novartis ran preclinical toxicology studies on STI-571 — the compound
that would eventually become imatinib (Gleevec) — across rats, mice, rabbits,
dogs, and monkeys. The dog studies returned a severe finding: significant liver
toxicity, including hepatocellular necrosis and bile duct changes. In many
programs, that finding ends the story. The compound dies.
What happened instead was mechanistic science working exactly as intended.
Toxicologists interrogated the species-specific finding, examined the primate and
human in vitro data, and determined that the hepatotoxic signal was not
reproduced in monkeys and did not translate to human biology. Rather than
abandoning the program, the team used that toxicological analysis to establish
appropriate clinical monitoring parameters and proceed with a defined risk
management framework.
The Phase I trial began in June 1998. By September of that year, investigators
noted that nearly every CML patient in the trial was responding. The FDA
approved Gleevec in May 2001 — the fastest cancer drug review in the agency’s
history at the time, just ten weeks after NDA submission. At five-year follow-up,
98 percent of chronic-phase CML patients remained in remission. A 2012
economic analysis estimated that the discovery and development of imatinib and
related drugs created approximately $143 billion in societal value.
That outcome was not guaranteed by the efficacy data. It was enabled by
mechanistic toxicology that distinguished a species-specific artifact
from a human risk signal — and translated that distinction into a governance
decision. Without it, one of the most transformative cancer drugs ever developed
might have been abandoned in 1996.
Toxicology did not just clear Gleevec for development. It saved it.
The failure pattern is consistent — and it is not scientific
Across the history of drug development, when toxicology fails, it tends to fail in
one of three ways. Each has a structural cause, not a knowledge cause.
- The translation failure (TGN1412, 2006)
TGN1412 was a CD28 superagonist monoclonal antibody that entered first-in-
human Phase I trials in the UK with a clean preclinical safety package. All six
healthy volunteers who received the drug developed life-threatening cytokine
release syndrome within hours, resulting in multi-organ failure. The non-human
primate studies had not predicted this. Not because the data were faked or the
scientists were careless — but because the species translation question for
immunomodulatory biologics had not been adequately interrogated. The
toxicology was compliant. The mechanistic question — how does the human
immune system respond to CD28 superactivation compared to the NHP model?
— was not resolved before first-in-human dosing.
The aftermath permanently changed how regulators approach first-in-human
starting doses for immunomodulatory biologics. The lesson is that for novel
modalities, regulatory compliance and scientific adequacy are not the same thing.
- The timing failure (FIAU, 1993)
Fialuridine was a nucleoside analogue antiviral in Phase II trials at NIH for
hepatitis B. Preclinical studies across multiple species showed no significant
toxicity. Then, patients in the trial began dying of acute liver failure and lactic
acidosis. Five patients died. Several required liver transplantation.
The mechanism, established later, was mitochondrial DNA toxicity — a
mechanism that accumulated only with sustained exposure and was not
reproduced in the standard animal models at standard durations. The toxicology
program had been compliant. It had not been mechanistically designed to catch a
cumulative, organelle-level target that manifests only after weeks of exposure.
FIAU redefined how pharmaceutical toxicologists think about nucleoside
analogues and mitochondrial liability, and spurred significant advances in
duration-sensitive toxicity screening. But it did so after five people died. - The late-signal failure (Thalidomide, 1957–1961; Troglitazone,
1997–2000)
These two cases sit decades apart but share a structural feature: the toxicity that
mattered most — teratogenicity in thalidomide, idiosyncratic hepatotoxicity in
troglitazone — was either not tested for under relevant exposure conditions or
was not detectable at the population sizes typical of clinical trials.
What saved the United States from the thalidomide catastrophe was not science
— it was governance. FDA reviewer Frances Kelsey withheld approval while
demanding adequate reproductive safety data at a time when the drug was
already being prescribed across Europe and Canada. Her refusal was an act of
toxicological governance: the absence of evidence of harm is not evidence of
absence, and the burden of proof belongs to the sponsor, not the regulator. The
1962 Kefauver-Harris amendments that followed codified this principle into law.
Troglitazone illustrates the limits of post-market surveillance as a safety system.
By the time the idiosyncratic hepatotoxicity signal was definitive, the drug had
been widely adopted, warnings had been added and ignored, and patients had
died. Withdrawal in 2000 came too late to prevent harm — and too late to be
anything other than a reactive measure.
What this means for founders, executives, and their investors
The governance implication of these cases is not that toxicology is magic or that
every adverse event is preventable. It is that organizations which treat toxicology
as a downstream compliance function systematically produce the same category
of outcome: a safety liability that surfaces after scale, after investment, and after
exposure — when the only levers left are withdrawal, litigation, and regulatory
damage control.
For biotech founders specifically, four practices separate programs that navigate
this well from those that do not:
- Build the toxicology hypothesis before you build the IND package. Know
what your compound’s primary mechanisms of concern are —
cardiovascular, hepatotoxic, immunotoxic, genotoxic — based on
structure-activity relationships and mechanistic class data, not just the
regulatory minimum study set. Your toxicologist should be informing
compound selection, not inheriting the selected compound. - Design studies to answer decision-relevant questions, not to satisfy
precedent. Regulatory tradition and scientific adequacy are not always the
same thing, as FIAU demonstrated. The question “what study does ICH
M3(R2) require?” and the question “what study would actually catch the
toxicity that could kill this program?” have overlapping but non-identical
answers. - Interrogate species translation for every novel modality. This is the
TGN1412 lesson. For biologics, gene therapies, EV-based therapeutics, and
other advanced modalities, regulatory compliance with standard primate
studies does not guarantee translational relevance. The mechanistic
question must be asked explicitly. - Treat toxicology uncertainty as a deliverable, not an embarrassment.
Uncertainty that is named, documented, and managed with a mitigation
plan is a program asset. Uncertainty that is unnamed because it is
inconvenient is a future liability.
For investors, the due diligence framing is simpler: ask whether the toxicology
strategy was designed to answer the most dangerous questions or designed to
achieve the minimum required to file. Those are different programs. Only one of
them knows what it does not know.
The thesis
The strongest version of this argument is not that toxicologists are smarter than
other scientists, or that other disciplines are incomplete. It is that toxicology is
the only discipline in the development process that is structurally required to
integrate mechanism, dose, duration, exposure, and defensible uncertainty into a
single decision object — and to do so before the harm occurs, not after it is
documented.
When that function is treated as a gate to pass rather than a source of insight, the
harm does not disappear. It migrates downstream, where it becomes more
expensive, more irreversible, and more visible.
Toxicology done early is R&D strategy. Toxicology done late is crisis
management. The science is the same. The cost is not.
Every organization that has paid the late-tox bill — in clinical failures, market
withdrawals, or litigation settlements — paid for the same thing they could have
bought earlier, at a fraction of the cost, before patients were exposed. The only
question is which version of that investment you choose to make.
Harriet Kamendi is a Regulatory Toxicologist and founder of Kandih Group, specializing in go-to-
market regulatory strategy, nonclinical safety program design, and pre-IND development for drug
and device programs.